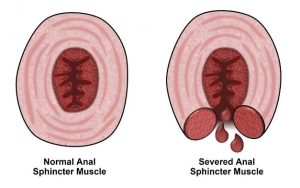
The anal sphincters constitute a set of 2 muscles that form a ring around the anus and are crucial in maintaining continence mechanism in the body. The anal sphincter is a complex muscular structure that comprises two main components: the inner, involuntary (smooth) muscle called the internal anal sphincter and the outer, voluntary (striated) muscle known as the external anal sphincterInternal Anal Sphincter: The internal anal sphincter is an involuntary muscle that remains contracted at rest. It serves as the primary barrier to prevent involuntary bowel movements. It’s crucial in maintaining continence by preventing fecal matter from escaping the rectum.
External Anal Sphincter: The external anal sphincter is a voluntary muscle that we can consciously control. It plays a secondary role in maintaining continence and allows us to voluntarily open the anus for defecation.
While the anal sphincter is a workhorse, injury or damage to the muscles can have significant consequences, such as:
- Fecal incontinence or leakage
- Pain
- Bleeding
- Perineal cellulitis
- Enteric fistulae
 A stay in the intensive care unit (ICU) can lead to fecal incontinence, as various medication, critical health conditions and other factors can cause diarrhea. Fecal incontinence can lead to skin irritation, breakdown and serious infections associated with cross-contamination due to fecal pathogens.
A stay in the intensive care unit (ICU) can lead to fecal incontinence, as various medication, critical health conditions and other factors can cause diarrhea. Fecal incontinence can lead to skin irritation, breakdown and serious infections associated with cross-contamination due to fecal pathogens.
ICU nurses frequently use intrarectal balloon catheters (IBCs) to manage fecal incontinent patients, but these devices can damage anal sphincter muscles. Since balloon catheters rely on inflating the balloon and a tonic sphincter, in some cases, nurses observe fecal leakage and spontaneous expulsions. To keep IBCs in place and to prevent potential leakage, users often fill the retention balloon with more liquid or air than recommended by the manufacturer. The practice is surprisingly common – in a recent study of 50 patients who had an IBC, over-inflation was the most common problem, with 14 percent of participants having an over-inflated retention balloon.
 When overinflated they exert high pressure at the increasing risk of sphincter dysfunction. Sphincter damage compromises the patient’s ability to control bowel movements, resulting in exacerbated fecal incontinence. Sphincter damage can weaken the support structures around the rectum, increasing the risk of rectal prolapse. This distressing condition involves the rectum protruding through the anus, leading to severe discomfort and complications. Patients with sphincter damage are more vulnerable to infections. The damaged tissue can serve as an entry point for pathogens, increasing the risk of incontinence associated dermatitis, blood stream infections, sepsis, and other complications.
When overinflated they exert high pressure at the increasing risk of sphincter dysfunction. Sphincter damage compromises the patient’s ability to control bowel movements, resulting in exacerbated fecal incontinence. Sphincter damage can weaken the support structures around the rectum, increasing the risk of rectal prolapse. This distressing condition involves the rectum protruding through the anus, leading to severe discomfort and complications. Patients with sphincter damage are more vulnerable to infections. The damaged tissue can serve as an entry point for pathogens, increasing the risk of incontinence associated dermatitis, blood stream infections, sepsis, and other complications.
Prolonged pressure on the rectal mucosa can cause tissue damage, leading to inflammation, irritation, and ulceration. In severe cases, excessive pressure from the balloon can cause tissue necrosis (cell death), often requiring additional medication, and even surgical intervention.
Each of these can cause systemic issues that can compromise patient health, extend stays, and even worsen fecal incontinence – sphincter damage from these complications can also increase the patient’s susceptibility to hospital-acquired infections (HAIs), also known as healthcare-associated infections.
Inappropriate use, improper insertion, overinflation of balloon catheters and leaving an IBC in too long can increase the risk for these complications.
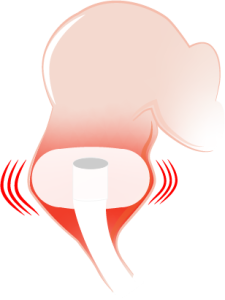
Qoramatic Soft Receptacle exerts 0 mmHg radial pressure
 Qoramatic is an industry first automated fecal management system that employs negative pressure suction to proactively divert fecal effluents. The device employs a soft teat/receptacle that exerts 0 mmHg radial pressure on the rectal mucosa minimizing any risk of rectal trauma, mucosal impairment, and injury. No inflation or over inflation, eliminates challenges and medical errors associated with high pressure balloons.
Qoramatic is an industry first automated fecal management system that employs negative pressure suction to proactively divert fecal effluents. The device employs a soft teat/receptacle that exerts 0 mmHg radial pressure on the rectal mucosa minimizing any risk of rectal trauma, mucosal impairment, and injury. No inflation or over inflation, eliminates challenges and medical errors associated with high pressure balloons.
Leakage is a common concern with intrarectal balloon catheters, but Qoramatic is designed to minimize the risk of leakage, reducing the chances of skin breakdown, pressure ulcers, and related hospital acquired infections. Efficient proactive fecal diversion helps reduce complications and discomfort, enhancing overall nursing satisfaction and superior clinical outcomes for patients.